Prioritization
Prioritization Considerations and Methods
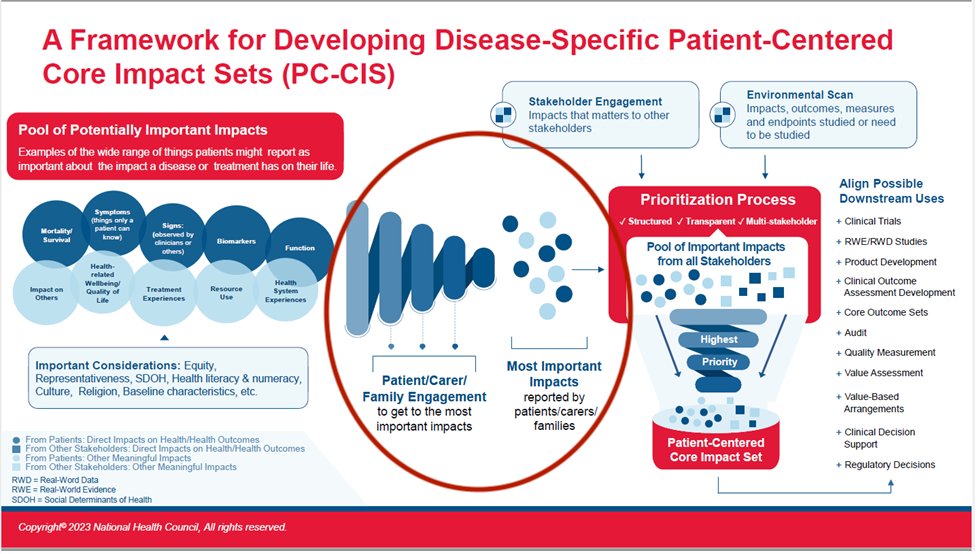
When the initial collection of patient-reported impacts happens, the breadth of what is reported will need to be prioritized to those impacts MOST important to patients before moving on to gathering data from other stakeholders. There are numerous methods that can be used in the prioritization process, and your research or methods partner(s) will likely have a preferred approach for such work.
Importantly, as Patient-Centered Core Impact Sets are an emerging and evolving tool, there is no proposed goal for the “ideal” number of prioritized impacts to arrive at. The expectation is that the correct number of impacts will vary by condition or population. In the development of the PC-CIS, the goal should be to compile the number of impacts representative of the full body of issues most important to patients and families. There is no gold-standard number.
Potential methods, examples, and guidance for prioritization include:
Delphi Method (panels and/or surveys)
- RAND Corporation Guidance
- INVOLVE UK Delphi Methods Description
- Systematic Review of patient participation in Delphi surveys to develop core outcome sets
Stated Preference Methods
- PATHWAY Programme Case Example
Nominal Group Technique
- Arthritis Foundation Live Yes! INSIGHTS Methodology Description
Discrete Choice Analysis
Mixed Methods
- Patient-Important Outcomes in the Long-Term Treatment of Bipolar Disorder Case Example
- PFMD Book of Good Practices and Patient Engagement Landscape paper (page 7)
- Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) Handbook Chapter 3
- The Core Outcome Set-STAdards for Development (COS-STAD) Guidelines for Core Outcome Set (COS) Guidelines for COS Development
Innovative Medicines Initiative (IMI), Patient Preferences in Benefit-Risk Assessments during the Drug Life Cycle (PREFER) Patient Preference Methodology
Arthritis Use Case
The nominal group technique steps used for the INSIGHTS program provides an example for how PC-CIS co-creation could occur, with very intentional and repeated involvement of patients/families in each step, even during more complicated elements of the project.
Patients and families were able to ask clarifying questions and gain more context when necessary, which allowed them to participate most fully in the discussion and process. The goal of these discussions was to collaborate fully with the participants rather than to conduct research on them.